




COVID19 – new threat, proven response
 COVID-19 is new – but an effective community response is the same.
COVID-19 is new – but an effective community response is the same.
The lessons from AIDS 1987-95 and Ebola 2014-15 still apply.
So, what can I do?
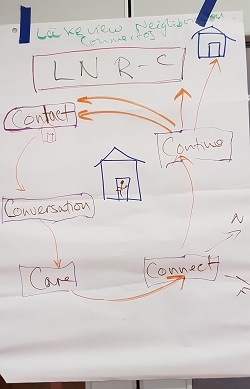
As ever, what matters most is local neighbourhood, and the basics of contacting, caring, conversing and continuing. It's called SALT practice – and it's how we work.
Indeed SALT is already at work, such as in Zambia's response.
SALT teams can be formed from among anyone who cares – from local entities such as schools and local neighbourhood support groups, or from churches, mosques and other faith interfaith groups.
 We must realise that everyone needs a conversation, and we must look for neighbourhood champions who are core connectors.
We must realise that everyone needs a conversation, and we must look for neighbourhood champions who are core connectors.
Through SALT activities we'll see trust-based friendship, confidence renewal, invitations to keep visiting, acts of love, being present, sensing love, seeing God, personally growing, and sharing prayer and faith.
Human contact must continue. We can still accompany our neighbours at a distance safe for sharing and listening, at doorsteps, streets and small gardens. This calms, reassures and connects, and brings hope and patience.
During the so-called lockdowns there are still legitimate ways and means of connecting with neighbours during a household group walk without having a group meeting.
Starting with people we may know a bit we pass by at a distance and the brief conversations expand, day by day.
This is true in any country with lockdown. We have to exercise our creative imagination and not lock down blindly by unwittingly choosing to understand it as isolation and separation.
Members of congregations can all be encouraged to contact nearby neighbours by passing by or dropping off something, showing care, then connecting those people up with others who can continue the accompaniment by phone or social media or passing by ... the point being that all streets, all small neighbourhoods have a champion who is the watcher, the carer, the changemaker, the innovator.
This has always been evident in poorer countries through HIV or Ebola response - but now we see it in USA, UK and Belgium etc. A global phenomenon.
Fairly soon the populations will be in two main groups ... the movers and the shielded. Neighbourhood connection becomes even more doable.
As we encourage local people in their own contexts they will create their own ways of responding and of supporting each other. We'll see them care and find hope.
Local and global conversations will need to connect with each other. Policy and practice at global and national levels will need to adapt and support.
And, of course, each country's systems will need to function, and need support, as do frontline health and others, including people of faith.
In Africa intense testing and contact tracing is really needed as the connector strategy for care and prevention, politics and the people, faith and health.
We will all be changed in our routines for many months. In our lifetimes we will find that the human experience is different forever. Outwardly, at least. Inwardly we have the chance to be transformed for the better.